Improving Care in Teens With Opioid Use Disorder
With opioid use disorder, a tiny fraction of young patients are getting treatment, which would not be acceptable for any other medical condition.


Maroke/AdobeStock

EXPERT Q&A
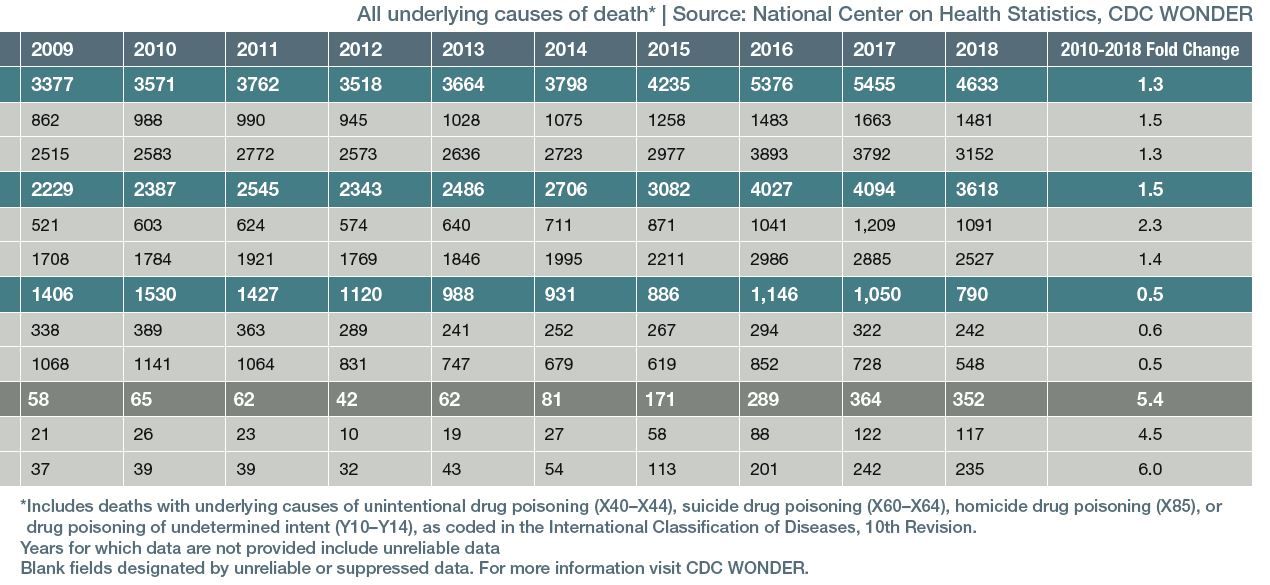
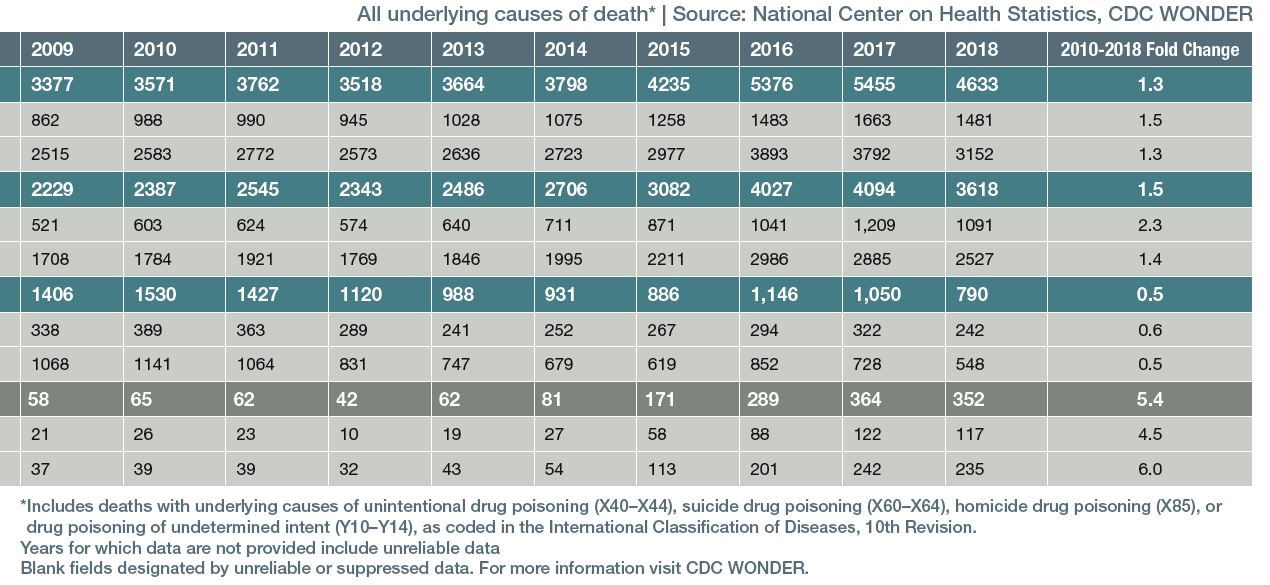
In the midst of a nationwide opioid epidemic, there is a population that is largely being ignored. According to a large cohort study, only a small percentage of teens receive proper aftercare following near-fatal overdoses. Alinsky and colleagues1 examined data from more than 4 million Medicaid enrollees (N = 4,039,216) and found that only 1 in 54 youths aged 13 to 22 years received evidence-based pharmacotherapy after an overdose. Unfortunately, it appears that proper care in this patient population is given in very few cases (Table 1A and Table 1B).
Psychiatric TimesTM invited lead author Rachel H. Alinsky, MD, MPH, to share insights from the study. Alinsky is an adolescent medicine and addiction medicine fellow at Johns Hopkins University School of Medicine in Baltimore, Maryland.
PSYCHIATRIC TIMESTM ( PT): Your research highlights the need for quality treatment, especially for younger patients. What insights can you provide about interventions and obstacles to treatment?


RACHEL H. ALINSKY, MD, MPH: We need to find effective interventions that can link adolescents and young adults directly into treatment after an opioid overdose. We also need to evaluate the barriers to accessing care at the time of overdose (such as insurance restrictions, lack of community providers or treatment centers, and stigma), and find strategies to mitigate these barriers. System-level changes are necessary, such as targeting federal funding for research and treatment for youth, decreasing insurance barriers, and increasing the availability of youth-serving physicians and addiction treatment centers.
PT: In the study, you and your colleagues noted, “Nonfatal opioid overdose may be a critical touch point when youths who have never received a diagnosis of opioid use disorder can be engaged in treatment.” Is that because these youths have hit rock bottom?
ALINSKY: In the addiction treatment field, we do not abide by that old adage—that people have to hit rock bottom before they are ready to get treatment. That is somewhat of a myth. What we are trying to emphasize in our article is that overdose is a particularly crucial time when we can draw someone into treatment because they are presenting into the medical setting, seeing doctors, and we have this opportunity to interact with them and offer them treatment. Coming into the emergency department with an overdose may be the only time this person is sitting face-to-face with a doctor, and we want to capitalize on this opportunity to offer the best care we can to the patient.
Of course, that does not mean they did not want treatment a month ago or a week ago—they very well might have wanted treatment but did not know how to access it in our very difficult-to-navigate addiction treatment system. So when the patient is physically with us after an overdose, we have the chance to help them gain access to lifesaving treatment.
PT: What are the key takeaway points from the study?
ALINSKY: Prior to this study, we knew that teens and young adults were about one-tenth as likely as adults to receive treatment for opioid use disorder in general.2 And while we knew that more than 4000 adolescents and young adults between the ages of 15 and 24 die from an opioid overdose every year,3 very little was known about health care use following nonfatal opioid overdose in youth. We were interested in figuring out the extent to which adolescents and young adults are receiving evidence-based treatment after a nonfatal opioid overdose.
We found that fewer than 1 in 50 adolescents and young adults who had an opioid overdose received the standard-of-care medication treatment that is recommended by the American Academy of Pediatrics.4 We also found that youths with opioid overdose have a high risk of recurrent overdose; more than 8% of youths with heroin overdose experience another overdose within 3 months.1
When an adolescent or young adult goes to the hospital with an emergency, you expect them to get the treatment they need. But here we see that less than 2% are getting that treatment, which would not be acceptable for any other medical condition. In pediatrics, it would be unacceptable if only 1 in 50 youths with asthma [received] the standard treatment when they came into the emergency department, or if 1 in 50 youths with diabetes [received] the standard treatment when they were hospitalized with diabetic ketoacidosis. Pediatricians would not find that treatment gap acceptable. Yet this is where we are now with the treatment for youths who have an opioid overdose—and we need to do better for them.
Additionally, with such high rates of recurrent overdose, it is even more important to get these youths into effective treatment as soon as possible, so we can try to prevent another overdose.
Finally, prescribing practices should be closely monitored in young people; they are a critically neglected patient population when it comes to addiction monitoring. As verified in an earlier study of 2,752,612 adolescents: “Safe opioid prescribing practices are critical to mitigate the risk of prescription opioid overdose in adolescents and young adults.”5
PT: What are the key issues in recognizing opioid use disorder in youth?
ALINSKY: The diagnosis of opioid use disorder is straightforward and is based on how many criteria an individual meets from a set of 11 criteria defined in DSM-5. In the case of youths who are presenting with opioid overdose, there is a chance that clinicians may view this as a standalone incident, and not recognize it as a manifestation of an adolescent’s underlying opioid use disorder. Thus, clinicians should be thinking about, and evaluating for, opioid use disorder in any youths that present with an overdose. Clinicians should probe for issues such as taking the opioid in larger amounts than intended, unsuccessful efforts to cut down use, cravings, recurrent use despite failure to fulfill obligations at school or home, or recurrent use in physically hazardous situations.
In terms of treatment, psychiatrists and other providers should offer medication for opioid use disorder as first-line treatment, consistent with recommendations from the American Academy of Pediatrics. These medications include buprenorphine, methadone, and naltrexone. Pharmacological interventions can be combined with behavioral health services such as therapy or counseling. The provider will need to determine the level of care that will best support the patient in their current stage of treatment—inpatient hospitalization, residential treatment, intensive outpatient, or outpatient treatment.
We know that medication is effective and lifesaving for opioid use disorder; large studies in adults have found that medication cuts the risk of death in half.6,7 We also know that youths who are on medication stay in treatment longer.8 Because so few youths actually ever receive this effective addiction treatment, an overdose can be an ideal opportunity to link someone into care who has not been able to access it previously.
PT: How can clinicians advise their patients and families on finding the most appropriate care?
ALINSKY: Patients and their parents can advocate for treatment by asking their doctors about treatment when they are in the emergency department with an overdose. Some emergency departments have programs where patients can immediately start on medication treatment; the programs can then link them to a provider in the community. These programs have been shown to be extremely effective, with much higher rates of individuals entering and staying in treatment than if someone is simply handed a phone number to call to set up treatment.9 If that sort of linkage is not available, families should ask to be referred so their teen or young adult can receive treatment in their community as soon as possible.
Clinicians or patients and families who want to find available treatment resources within their community can use the treatment locator provided by the Substance Abuse and Mental Health Services Administration (https://findtreatment.samhsa.gov/). Here you can enter your zip code and find all the available addiction treatment centers, sorting by services offered. It is also possible to specifically look for buprenorphine prescribers or methadone programs from that web page.
References
1. Alinsky RH, Zima BT, Rodean J, et al. Receipt of addiction treatment after opioid overdose among Medicaid-enrolled adolescents and young adults. JAMA Pediatr. 2020;174(3):e195183.
2. Chua KP, Brummett CM, Conti RM, Bohnert A. Association of opioid prescribing patterns with prescription opioid overdose in adolescents and young adults. JAMA Pediatr. 2020;174(2):141-148.
3. Overdose death rates. National Institute on Drug Abuse. Updated March 10, 2020. Accessed November 30, 2020, 2020. https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates
4. Committee on Substance Use and Prevention. Medication-assisted treatment of adolescents with opioid use disorders. Pediatrics. 2016;138(3):e20161893.
5. Feder KA, Krawczyk N, Saloner B. Medication-assisted treatment for adolescents in specialty treatment for opioid use disorder. J Adolesc Health. 2017;60(6):747-750.
6. Larochelle MR, Bernson D, Land T, et al. Medication for opioid use disorder after nonfatal opioid overdose and association with mortality: a cohort study. Ann Intern Med. 2018;169(3):137-145.
7. Medications for Opioid Use Disorder Save Lives. The National Academies Press. Accessed November 30, 2020. http://www.nationalacademies.org/hmd/Reports/2019/medications-for-opioid-use-disorder-save-lives.aspx
8. Hadland SE, Bagley SM, Rodean J, et al. Receipt of timely addiction treatment and association of early medication treatment with retention in care among youths with opioid use disorder. JAMA Pediatr. 2018;172(11):1029-1037.
9. D’Onofrio G, O’Connor PG, Pantalon MV, et al. Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial. JAMA. 2015;313(16):1636-1644.❒