










Personality disorders are arguably the most challenging for psychiatrists because they are difficult to diagnose and frequently coexist with psychotic, affective, and anxiety disorders.
Personality disorders are arguably the most challenging for psychiatrists because they are difficult to diagnose and frequently coexist with psychotic, affective, and anxiety disorders.

Despite the disappearance of identity variations in diagnostic classifications, psychiatrists can contribute to solving social challenges.

The key focus is on understanding violent offending (eg, reactive, proactive, firearm violence) tied to antisocial personality disorder and psychopathy using a psychobiological lens.
This study highlights the need to consider a holistic approach when discussing the problem of disruptive behavior in health care settings.

The psychopath has the image of a cold, heartless, inhuman being. But do all psychopaths show a complete lack of normal emotional capacities and empathy?
This exchange follows what began with Dr Richard Noll’s article, “Speak, Memory” and the “repressed recovered memory/multiple personality disorder” iatrogenic epidemic of the late 1980s and 1990s.
How the Repressed-Recovered Memory–Multiple Personality Disorder iatrogenic epidemic-surely one of the most tragic chapters in the history of psychiatry, psychology, and psychotherapy-ended, and how psychotherapy patients came to be protected by informed consent.
What factors are involved in parents’ decision to begin medication treatment for a child with ADHD? An overview of studies that provide clinically relevant information related to the course and treatment outcomes of ADHD in children and adolescents.
In the 1980s, thousands of patients insisted they were recovering childhood memories of physical and sexual abuse during Satanic cult rituals. Here: a look back at the moral panic.
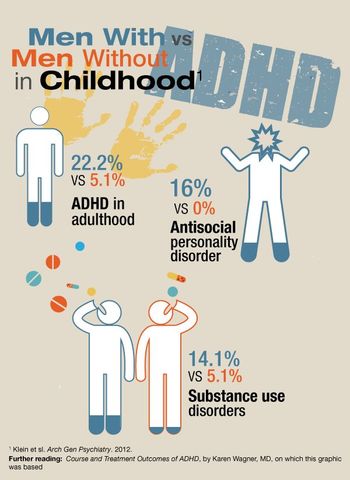
The results of the study featured in this infographic showed that compared with men without childhood ADHD, men with childhood ADHD had higher rates of ongoing issues in adulthood.
There are many stories written about serial killers and murderers, books that narrate the life course of individuals who commit heinous acts. However, few have been written by murderers explaining their lives first-hand.
To understand the psychodynamics of the dissociative fugue, Dr Michael Sperber analyzes some of the characters in a collection of interrelated vignettes set in small town America.

Patients with borderline personality disorder or narcissistic personality disorder (or both) can feel entitled to special treatment and often seek only approving forms of attention from those who treat them.

Adjustment disorder is one of the few psychiatric diagnoses for which the etiology, symptoms, and course, rather than symptoms alone, are central to making the diagnosis. Both emotional and behavioral disturbances are present and include low mood, tearfulness, anxiety, self-harm, withdrawal, anger, and irritability.

People who weren't getting out of bed are getting up and doing productive things. They are re-engaging with their families, and they are focusing on things they want to accomplish before they die.

Borderline personality disorder typically coexists with depression, anxiety, and substance abuse. Symptoms of these conditions may lead the clinician to miss the diagnosis of personality disorder entirely. Careful diagnosis of BPD and comorbid disorders is the first step.
What we know for sure is that for all the young children and adults who were killed in Newtown, their world ended a week ago. Soon after the tragedy, one of the fathers of a child killed tearfully pleaded for society to learn from what happened in order to prevent future mass murders. Here, recommendations from a psychiatrist.

Therapy is a matter of cleaning the dust off so that you can see what's underneath.

Assessments of partial culpability of adolescents are difficult in individual cases; however, the courts are moving away from mandatory sentencing to individual determinations, even for the most heinous crimes.

Traumatic brain injury (TBI) in children and adolescents is a major public health problem. Psychiatrists have a crucial role in the management of young persons who have a TBI.
If we, as a people, continue to sacrifice genuine security for a false sense of freedom, we shall find ourselves in a nation neither secure nor free.

"You turn on the television, and violence is there. You go to a movie, and violence is there."

The article focuses on eating disorders in males and presents information on similarities and differences between males and females as they relate to risk factors, clinical presentation, and treatment.

Boys with ADHD can present with different cognitive and behavioral patterns than girls with ADHD. Despite these factors, girls with ADHD remain at significant psychosocial risk into adulthood.

In this review, we discuss the established medications as well as experimental therapeutic options that may emerge as future medications for alcohol intoxication, withdrawal, and/or long-term abstinence maintenance or harm-reduced drinking.