

Publication
Article
Psychiatric Times
The Final “P” in Pain Management
Author(s):
With a broader and multifaceted understanding of pain, patient care can move from a focus on eradicating pain, as based on objective pain scores, to improving the patient’s quality of life, while simultaneously decreasing pain to a level that is acceptable to the individual patient.


ST.art/AdobeStock

The English word pain is derived from the Latin word poena, meaning penalty or punishment. Because of the intrinsically intimate and subjective nature of pain, philosophers and medical providers struggle to find a definitive definition of the word. It is variable through references, authors, and times, with conceptualizations focusing alternately on the biomedical, emotional, or behavioral components of the phenomenon. The philosopher René Descartes’ mechanistic conceptualization of pain as a sensation, where the animal merely reacts to the noxious stimulus, dominated scientific and folk beliefs about pain into the mid-20th century.1 The more modern emergence of the concept of being-in-pain, which includes the subjectivity of the individual in the experience, opens the door for a bigger involvement of mental health professionals in pain management.
To conceptualize this understanding, the International Association for the Study of Pain coined a new definition of pain in 1979: “unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.”2 This flexible definition acknowledges the sensory, cognitive, affective, and motivational processes that influence the experience of pain and allows for a broader exploration of its subjectivity. It trades a purely neurological view for a more holistic conceptualization that considers the totality of the pain and, more importantly, of the patient.3
The differentiation between acute and chronic pain has proven to be clinically useful for tailoring interventions. Traditionally, the distinction between acute and chronic pain has relied upon a single continuum of time, with the designation of an arbitrary interval as a transition point, most commonly between 3 and 6 months. Another way to characterize chronic pain is pain that extends beyond the expected period of healing—assuming one knows what that should be.
Both acute and chronic pain are major public health problems with high health care costs and resource requirements. According to a study published in 2012, the conservative estimate of the health care cost of pain is around $560 to $635 billion annually, which is significantly greater than that of heart disease, cancer, or even diabetes mellitus.4 Because of this high prevalence and significant morbidity, pain has earned the designation of “the fifth vital sign.”
Despite these tremendous expenses and heroic efforts (using sophisticated technology, biomedical advances, and ever-growing research), most pain conditions have no final options for a cure. The only potent analgesics available are opioids, which can be problematic given the current opioid epidemic in Western countries. However, with the broader and multifaceted understanding of pain, patient care has moved from a focus on eradicating pain, as based on objective pain scores, to improving the patient’s quality of life, while simultaneously decreasing pain to a level that is acceptable to the individual patient. To achieve this goal, the clinical integration of mental health providers in pain management teams has become more widespread.
The Relationship Between the Experience of Pain and Mental Health
If we agree with Ludwig Wittgenstein, PhD, who posited that “words are connected with the primitive, the natural expressions of the sensations and are used in their place,”5 it is not hard to see that even in the everyday language about pain, there exists a significant overlap between the purely physical experience of pain and the consequent subjective emotional aspects that arise with it. It might even seem that the connection transcends all elaborate philosophical theories and is deeply felt and expressed on an instinctual level. The most obvious example of the connection is that expressions like “broken-hearted” or “a slap in the face” are often used in multiple languages to describe experiences of physical as well as emotional, psychological, or even spiritual suffering.
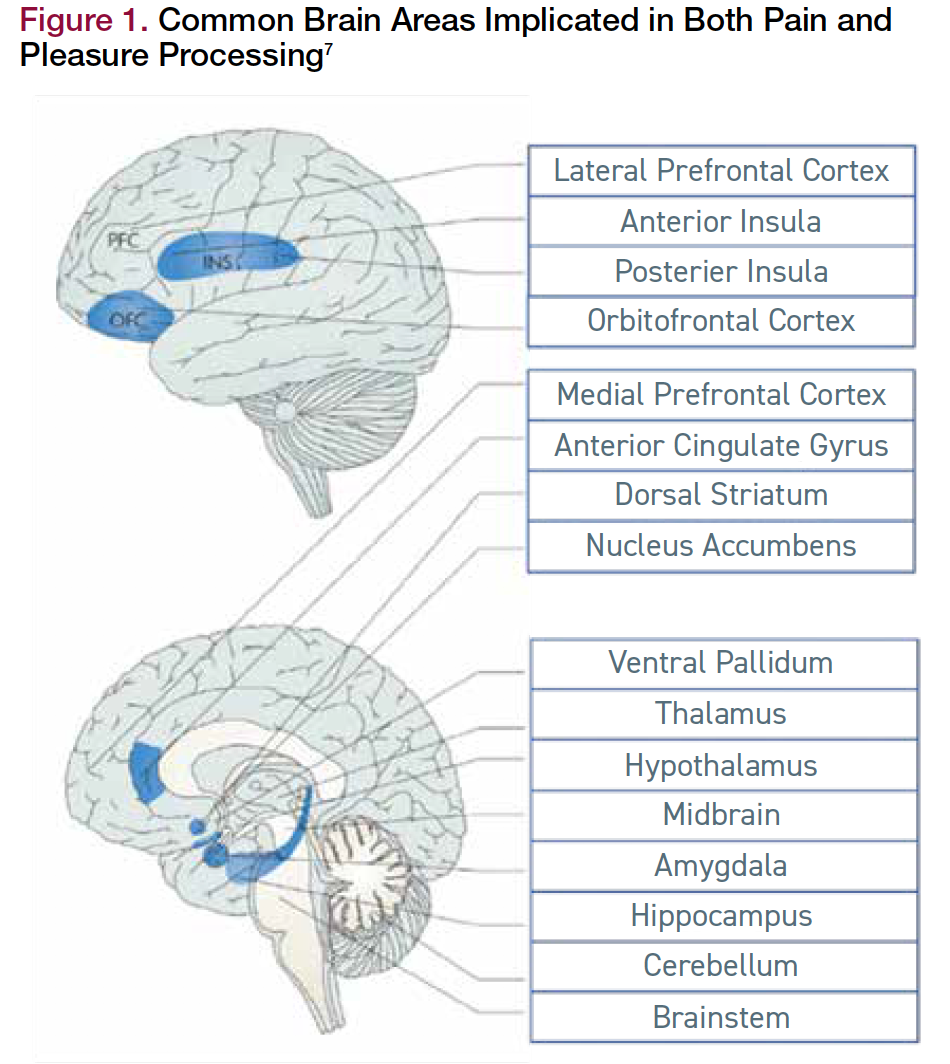
This intimate and intricate relationship is also well understood even if one chooses to look at it from a purely neurobiological perspective. Although pain might initially originate from peripheral sensory receptors, the experience of pain is not complete without the modulatory involvement of the central nervous system.6 Afferent stimuli from the thalamus, the limbic system, and cortical structures like the frontal lobe and the somatosensory cortex amplify or diminish the peripheral painful stimuli and add a subjective emotional component to the sensation. Functional imaging techniques and direct brain stimulation studies have demonstrated a striking overlap between central structures implicated in the processing of pain and reward (Figure 1).7 In addition, recent studies have described how chronic pain changes grey matter in the brain, resulting in secondary psychiatric symptoms and disorders. These studies thus emphasize a bidirectional relationship between pain and psychiatric disorders.8


Figure 1. Common Brain Areas Implicated in Both Pain and Pleasure Processing7
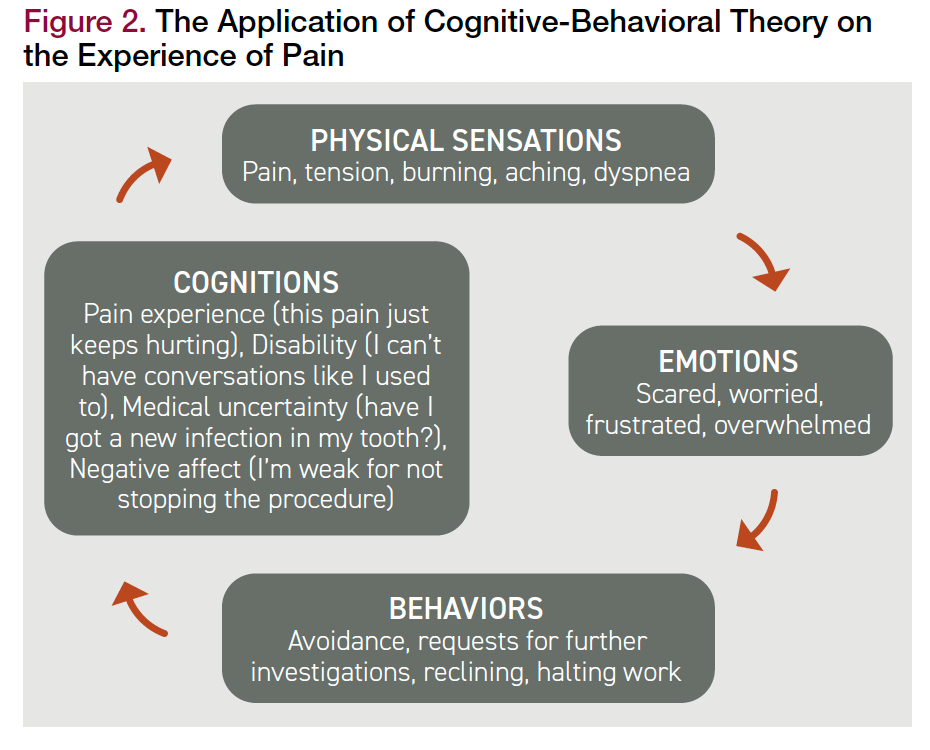
An individual’s experience of pain cannot be understood in a sterile context. With this conceptualization comes the possibility of applying psychological principles to the treatment of pain. Cognitive behavioral theories of pain are based on the premise that cognitions, emotions, behaviors, and physical sensations are all interrelated and exist within a particular context.9 Psychologists observe that changes in any of these areas can have wide-ranging influences through a circular effect on each other.
The diagram in Figure 2 illustrates how the different components of cognitive behavioral therapy (CBT) interact with each other to create vicious cycles, which in turn can cause a clinical increase in symptoms. From an interpersonal perspective, it is also clear that persistent personality traits can influence the subjective experience and expression of pain. Specific defensive and coping styles in an individual may create a particular and sometimes stereotyped experience of pain.10 Finally, although there is limited interest in the psychodynamic perspective of pain, multiple authors have argued that patients communicate on multiple conscious and unconscious levels through bodily manifestations, and that pain expressions hold symbolic latent meanings that warrant psychological and psychoanalytic exploration.11


Figure 2. The Application of Cognitive-Behavioral Theory on the Experience of Pain
The Empirical Evidence for an Interdisciplinary Approach to Chronic Pain
From a more practical standpoint, evidence-based medicine shows a significant association between pain and mental health disorders and symptoms. There exists a statistically important comorbidity between acute and chronic pain and depressive disorders, anxiety disorders, substance use disorders, and personality disorders.12,13 Empirical evidence shows higher efficacy for the multidisciplinary and interdisciplinary management of pain that is based on the biopsychosocial model, which combines physical therapy, pain management by medication, patient education, ergonomic training, psychiatric treatment, and psychotherapy, among others. These interventions have shown significant results on the ratings of pain intensity scores, as well as on the quality-of-life measures that encompass both mental health and the functional impacts.14,15
The Role of the Consultation-Liaison Psychiatrist in the Management of Pain
Consultation-liaison (C-L) psychiatrists are key members and leaders of interdisciplinary pain management teams. Psychiatry residents get the most training in pain management during the substance abuse/addictions (60%) and the C-L psychiatry (57%) rotations.16
C-L psychiatrists are uniquely qualified to help patients with pain and play an important role in the pain management team. Although most primary care physicians and medical specialists can diagnose and initiate the treatment of psychiatric disorders, C-L subspecialists can diagnose more subtle and complex mood or anxiety disorders, substance use disorders, or personality disorders in a general medical setting. They can also participate in the pharmacological and even interventional management of pain, detect possible drug-drug interactions in these medically complex patients, and screen for possible medication side effects.
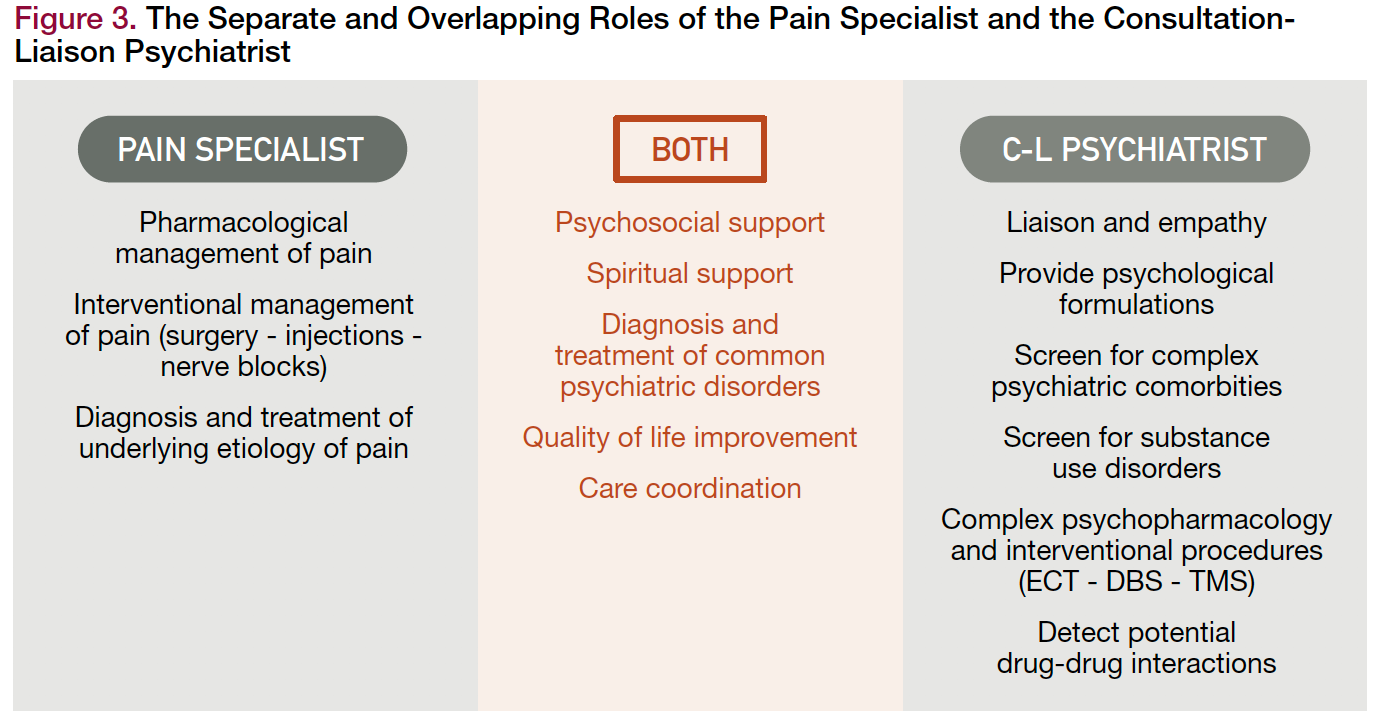
In addition, as the name of the specialty reveals, C-L psychiatrists are experts in bridging the gap between the patient and the other medical teams. They can relay messages in an empathic and understanding way and bring the goals of treatment into alignment with the patient’s values, preferences, and styles. Their integrated view of patients allows for reflection on behavioral, interpersonal, and psychodynamic formulations of the patient’s pain experience that can be communicated to the team to personalize the treatment and thus improve the quality of the care. Figure 3 details the separate and overlapping roles of the pain specialist and the C-L psychiatrist.


Figure 3. The Separate and Overlapping Roles of the Pain Specialist and the Consultation Liaison Psychiatrist
Exploring the Future of C-L Psychiatry Within Pain Management Teams
In 2019, a study published in Pain Medicine showed a national improvement of pain education in psychiatry training.17 The investigators found that more than two-thirds (70%) of program directors supported having psychiatry residents receive education and training in chronic pain management. This is a significant improvement from the less than 50% found in the 2012 survey by Hagstrom et al.16
The increase in pain management education is not limited to psychiatry residency; it also currently includes more continuing medical education (CME) focused on psychiatric aspects of pain, medication management of pain, meditation, CBT, and other strategies.18 This is particularly true for C-L psychiatrists, whose national professional organization, the Academy of Consultation-Liaison Psychiatry, specifically includes CME for chronic pain as well as special interest groups for palliative medicine, addiction and toxicology, and collaborative and integrated care, among others.19
Overall, the future of this integrated approach to pain with the inclusion of C-L psychiatrists looks bright. Encouraging systemic changes are starting to occur, including changes to reimbursement for medical services (meaning procedural and nonprocedural pain interventions will be more equally compensated). They also include changes to the referral processes between specialists, making the processes more efficient and allowing the emergence of bigger interdisciplinary teams.
We believe that an integrated treatment actively involves C-L psychiatry which, in the words of Elman et al, constitutes the final missing P in the management of pain,20 and which can significantly improve health outcomes and the quality of life of this patient population.
Dr Noufi is a consultation-liaison psychiatrist and palliative care fellow at MedStar Washington Hospital Center in Washington, DC. Dr Pao is clinical and deputy scientific director of the National Institute of Mental Health and the National Institutes of Health, and acting clinical director of the National Center for Complementary and Integrative Health, all in Bethesda, MD.
References
1. Descartes R. Meditations on First Philosophy: With Selections From the Objections and Replies. Moriarty M, trans. Oxford University Press; 2008.
2. Treede R-D. The International Association for the Study of Pain definition of pain: as valid in 2018 as in 1979, but in need of regularly updated footnotes. Pain Rep. 2018;3(2):e643.
3. Mehta A, Chan LS. Understanding of the concept of “total pain”: a prerequisite for pain control. J Hospice Palliative Nurs. 2008;10(1):26-32.
4. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715-724.
5. Wittgenstein L. Philosophical Investigations. Anscombe GEM, trans. Wiley-Blackwell, 1997.
6. Elman I, Borsook D, Volkow ND. Pain and suicidality: insights from reward and addiction neuroscience. Prog Neurobiol. 2013;109:1-27.
7. Leknes S, Tracey I. A common neurobiology for pain and pleasure. Nat Rev Neurosci. 2008;9(4):314-320.
8. May A. Chronic pain may change the structure of the brain. Pain. 2008;137(1):7-15.
9. Penlington C, Urbanek M, Barker S. Psychological theories of pain. Prim Dent J. 2019;(7)24-29.
10. Naylor B, Boag S, Gustin SM. New evidence for a pain personality? a critical review of the last 120 years of pain and personality. Scand J Pain. 2017;17:58-67.
11. Jimenez XF. Parallel pains and dynamic dilemmas: psychodynamic considerations in approaching and managing chronic physical pain. Psychodyn Psychiatry. 2019;47(2):167-182.
12. Velly AM, Mohit S. Epidemiology of pain and relation to psychiatric disorders. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):159-167.
13. Ilgen MA, Kleinberg F, Ignacio RV, et al. Noncancer pain conditions and risk of suicide. JAMA Psychiatry. 2013;70(7):692-697.
14. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
15. Gerdle B, Åkerblom S, Brodda Jansen G, et al. Who benefits from multimodal rehabilitation - an exploration of pain, psychological distress, and life impacts in over 35,000 chronic pain patients identified in the Swedish Quality Registry for Pain Rehabilitation. J Pain Res. 2019;12:891-908.
16. Hagstrom AK, Leo RJ, Breitborde N. The status of pain medicine education in psychiatry: a survey of residency training program directors. Acad Psychiatry. 2012;36(1):66-68.
17. Majeed MH, Ali AA, Metzger S, Sudak DM. Pain management education and training during psychiatry residency: a report on national progress. Pain Med. 2019;20(12):2346-2348.
18. Balon R, Morreale MK, Coverdale JH, et al. The role of psychiatric education in pain management. Acad Psychiatry. 2018;42(5):587-591.
19. Academy of Consulation-Liaison Psychiatry. CLP 2020: delivering our vision of integrated care. 2020. Accessed March 22, 2021. https://www.clp2020.org/
20. Elman I, Zubieta JK, Borsook D. The missing p in psychiatric training: why it is important to teach pain to psychiatrists. Arch Gen Psychiatry. 2011;68(1):12-20. ❒














Newsletter
Receive trusted psychiatric news, expert analysis, and clinical insights — subscribe today to support your practice and your patients.







