Publication
Article
Psychiatric Times
Is It OCD or an Anxiety Disorder? Considerations for Differential Diagnosis and Treatment
Author(s):
While it may be challenging to differentiate between OCD and other anxiety disorders, using a multi-informant assessment and understanding the content of a patient’s fears is a fundamental start to outlining an effective treatment plan.





Table. Differentiating between non-OCD and OCD presentations
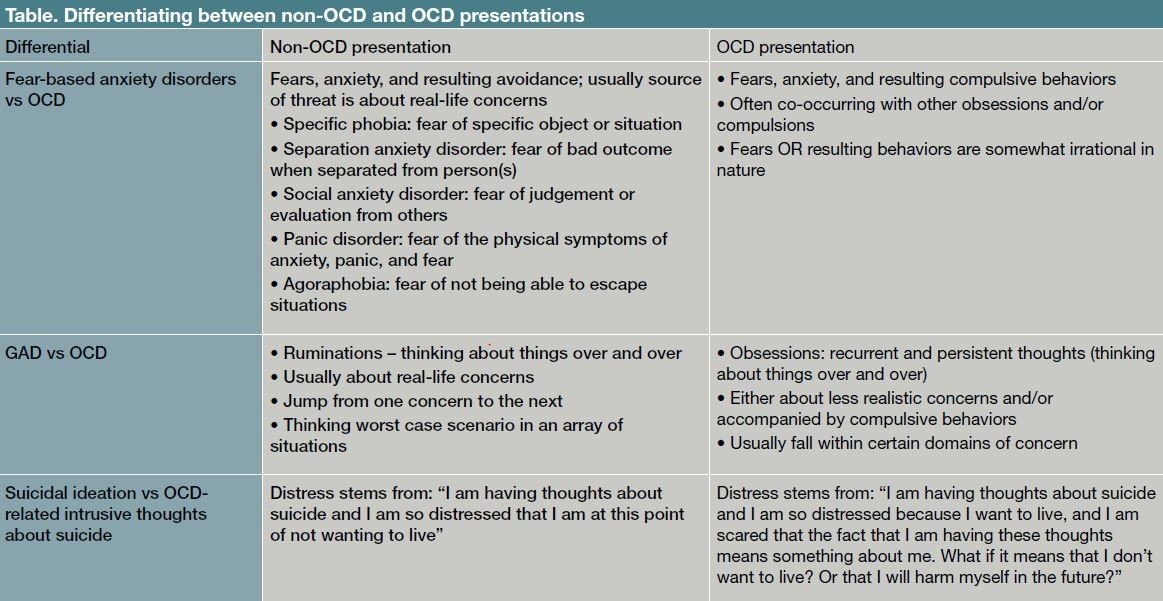


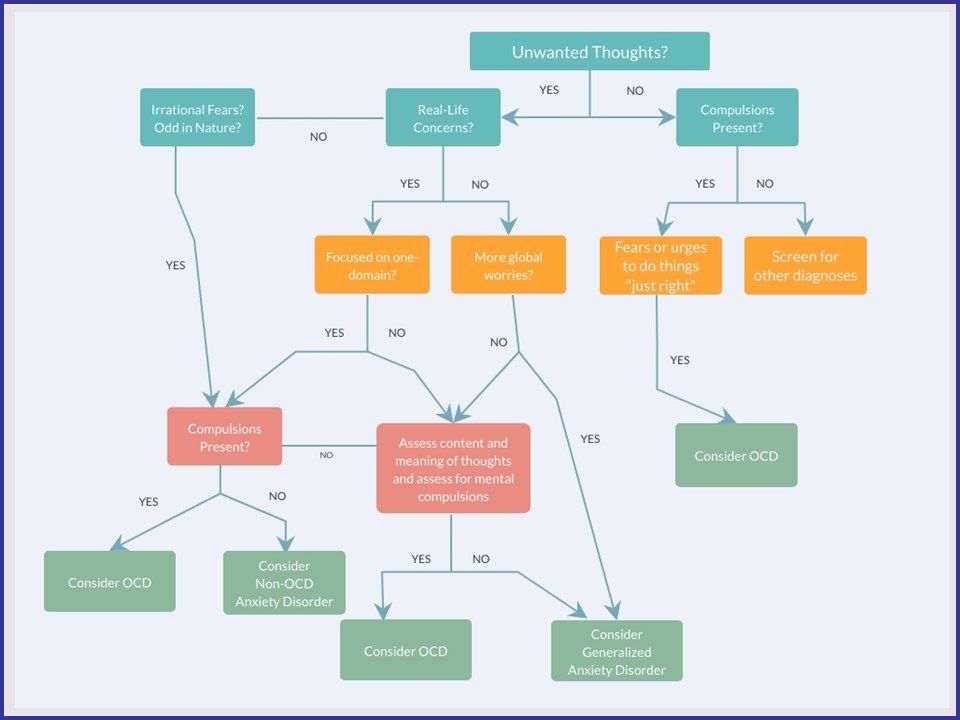
Figure. Determining whether it is OCD
SPECIAL REPORT: OCD AND RELATED DISORDERS
OCD manifests as recurrent and persistent obsessive thoughts, and/or repetitive compulsive behaviors. The disorder affects about 2% of the population, with incidence peaks in both pre-adolescent children, and young adults.1 Anxiety disorders are the most common emotional difficulty for children, and in the in the US, 7.1% of children (aged 3-17 years) have been diagnosed with an anxiety disorder.2 This number increases when considering lifetime prevalence, and up to one-third of the population will suffer from an anxiety disorder at some point.3 OCD and anxiety disorders present differently from child to child, and it can be challenging to distinguish between the various anxiety disorders and OCD. While anxiety disorders and OCD are often comorbid, and have overlapping symptoms, there are some key distinguishing factors that lead to diagnostic clarity.4 Differentiating between these attributes can guide treatment choices and goals for OCD as well as non-OCD anxiety disorders.
Differential diagnosis
In 2013, DSM-5 separated OCD from anxiety disorders by creating a distinct category of Obsessive Compulsive and Related Disorders. While the diagnostic criteria spell out differences between the categories, phenotypically, the presentations of OCD and anxiety disorders, such as social anxiety disorder and specific phobias, can appear very similar.
DSM defines obsessions as “recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress.” This marked anxiety or distress leads to an urge to complete compulsions. Patients often come in describing that they are “obsessing,” or having persistent thoughts, yet, these descriptions do not necessarily indicate the presence of OCD and may be indicative of ruminations or fears more consistent with an anxiety disorder.
Two helpful considerations when determining whether recurrent thoughts are obsessions as defined within the framework of OCD are the source of the threat and the nature of the thoughts as well as presence or absence of compulsive behaviors.
1. The Source of Threat and Nature of the Thoughts. The source of threat can help distinguish between the various anxiety disorders. According to DSM, the presence or absence of “non-real-life concerns” or content that is “odd, irrational, or of a seemingly magical nature” can often indicate OCD. DSM-5 added the possibility that an individual may not recognize that the beliefs are possibly untrue, and in this case, there is a specifier “with absent insight/delusional beliefs.”
2. Compulsive Behaviors. There are instances in which the obsessions are about something rational; however, in these cases, there are often rituals or compulsions that are not rational responses to the thought. While DSM 5 does not require that the individual recognize that the behaviors are irrational, the criteria still clearly states “these behaviors or mental acts are not connected in a realistic way with what they are designed to neutralize or prevent, or are clearly excessive.”
Case Vignette
Max is terrified of vomiting. He avoids being near sick people and runs away when he hears that someone in his class has been ill.
Sarah is also terrified of vomiting. She engages in excessive and ritualized hand washing to prevent illness, and her hands are chapped and raw as a result. She counts the number of seconds she washes to make sure she feels that she has completed her cleaning task.
In a specific phobia, there may be recurrent thoughts about a specific topic or item. It may appear that these are “obsessions.” In both of these examples, we can consider that the source of threat-illness and vomiting-is the same. This is not a nonâreal-life concern and the content is not odd, irrational, or of a seemingly magical nature. With Max, rituals are not present, and instead we see significant avoidance. Only Sarah presents with compulsions, which are not connected in a fully realistic way with the prevention of illness.
We can extend this example to other anxiety disorders: in a case of social anxiety disorder, the source of threat is judgement and evaluation from others. A person may have recurrent thoughts about this but typically engages in avoidance of these situations rather than in compulsive behaviors that are disconnected with the fear. In generalized anxiety disorder, a person is likely to have recurrent and persistent thoughts about a variety of things, yet these are categorized as ruminations. If the person has compulsions, then this may warrant a separate diagnosis of OCD (Table).
Case Vignette
Jamie is having recurring thoughts about harming herself and others. She is terrified to go near knives, for fear that she will hurt someone. She is extremely distressed about these thoughts and seeks reassurance to confirm that she has not hurt anyone from her mother multiple times a day.
Danielle has suffered from OCD symptoms for years. She is now presenting with significant symptoms of depression and is having thoughts about harming herself. She is distressed about the fact that she is having suicidal ideation and hates that she is having so much trouble finding a reason to live.
Both Jamie and Danielle present with thoughts about harming themselves, and in both cases, these thoughts are distressing. The differential that we are considering is whether these thoughts are intrusive thoughts consistent with OCD, or true suicidal ideation.
Intrusive thoughts are unwanted thoughts that a person does not agree with.5 The thoughts are most often incongruent and antithetical to the person’s values and true beliefs. Jamie is having thoughts about harming others even though she absolutely does not want to, and she is even horrified by the thought. A person may have thoughts about sexual interest in children, even though he or she are not interested in children sexually. These are intrusive thoughts, and the obsession and source of threat is “does the fact that I am having a thought mean something about me?” or “does the fact that I am having a thought mean something about my desires and what I may do in the future?”
The thoughts are taken as truth and are often interpreted as holding significant meaning about the individual. With intrusive thoughts, a person often does not understand why they are having these thoughts. The thoughts are ego-dystonic, and often the opposite of the individual’s desires.
Case Vignette
Jamie is having recurring thoughts about harming herself and others. She is terrified to go near knives, for fear that she will hurt someone. She is extremely distressed about these thoughts and seeks reassurance to confirm that she has not hurt anyone from her mother multiple times a day.
Danielle has suffered from OCD symptoms for years. She is now presenting with significant symptoms of depression and is having thoughts about harming herself. She is distressed about the fact that she is having suicidal ideation and hates that she is having so much trouble finding a reason to live.
In contrast, Danielle is distressed about her thoughts of harming herself, but she is further distressed because she has some ego-syntonic desire to harm herself. Fears may also be ego-syntonic. A fear of being stabbed by an intruder is consistent with what a person wants: a desire to prevent being stabbed. In many cases, this would be categorized as a fear, and may be consistent with a phobia or anxiety disorder.
Treatment strategies
In Jamie’s case, we would provide psychoeducation about intrusive thoughts and OCD, and then proceed to exposure and response prevention. We would have her face her obsession that her thoughts are meaningful by purposely thinking about harming people, while preventing any reassurance seeking and avoidance. We would also have her hold knives while thinking these thoughts. This would allow her to see that her thoughts are not dangerous, and do not reflect who she is or who she will become. She will learn that she can think the thought, and still not harm anyone. For Danielle, despite her significant history of OCD, we would address her primary concern of depression and suicidal ideation.
Case Vignette
Ben has a life-threatening allergy to nuts and is terrified of having a severe allergic reaction. Upon further assessment, Ben explains that he has stopped eating at restaurants, even when they are nut-free, and checks food labels multiple times, even on products that he has previously eaten. His mother discloses that, a few years ago, he washed his hands five times before each meal.
When it remains unclear whether a presentation is OCD or an anxiety disorder, it may be helpful to assess for other compulsive behaviors, past or present. Ben presents with fear of an allergic reaction, which could be a specific phobia. Upon further assessment, you find out that there are current checking behaviors that are irrational. Even if these were not present, the history of hand-washing compulsions is a strong indicator that Ben’s symptom presentation is likely consistent with a diagnosis of OCD (Figure).
When considering a course of treatment, it is helpful to conceptualize OCD separately from anxiety disorders, from both psychotherapeutic and medication perspectives. Anxiety disorders are treated with cognitive behavioral therapy (CBT), which includes exposure, facing fears and anxiety provoking situations. With anxiety disorders, this exercise revolves around facing the fears themselves. When treating OCD, this treatment element is part of exposure and response prevention.
Preventing a compulsion or compensatory behavior is essential. If a person completes exposures, but later engages in the compensatory behaviors, rituals, or compulsions, the individual learns that they are only okay because they completed the compensatory behavior. The impact of the exposure is diminished, and this reinforces the obsessive-compulsive cycle, rather than reducing it. For example, if a patient has OCD with contamination concerns, and he practices touching the floor throughout his session, but then goes home and scrubs his hands for 30 minutes, he only learns that he was able to tolerate the exposure because he was able to complete a compulsion. Treatment for OCD must include both the exposure AND the response prevention.
The first-line medications for both OCD and anxiety disorders are SSRIs. Additionally, for both OCD and anxiety disorders there is strong evidence for a combination of SSRIs and CBT as the most effective treatment.6,7 However, despite strong evidence of the effectiveness of SSRIs in the treatment of anxiety, the only FDA-approved medication for childhood anxiety disorders is the SNRI, duloxetine for treating generalized anxiety disorder.8 The evidence for the use of alternative medications including venlafaxine, buspirone, mirtazapine, tricyclic antidepressant, and benzodiazepine among others, is less compelling or negative.8,9
This is not the case for OCD; fluoxetine, sertraline, fluvoxamine, and clomipramine are all FDA-approved for the treatment of pediatric OCD giving clinicians numerous options before considering off-label treatments. When treating OCD with medication there are two additional major differences. OCD often requires high doses of SSRIs, doses that are not usually necessary for anxiety disorders. Moreover, OCD may take longer to respond to medications than anxiety disorders and so clinicians must prepare their patients for this and understand this before deciding to further titrate a patient’s dose of medication.
Differential diagnosis is also critical to medical decision-making as certain comorbid disorders (eg, tic disorders) may affect the choice and response to medications. For example, patients with co-occurring tic disorders and OCD may benefit more from off-label augmentation with an atypical antipsychotic than patients who do not have a tic disorder.
Conclusions
While it may be challenging to differentiate between OCD and other anxiety disorders, using a multi-informant assessment and understanding the content of a patient’s fears is a fundamental start to outlining an effective treatment plan. It is also important to consider that given the high comorbity between anxiety disorders and OCD, if a patient meets full criteria for both OCD and an anxiety disorder both diagnoses should be given.
Treatment approaches for anxiety disorders emphasize aspects of exposure treatment, and it is essential to include response prevention in the treatment of OCD. Maintaining an openness to the source of threat and presence of less typical symptoms as you assess and build rapport with a patient can aid in diagnostic clarity and provide a foundation to flexibly adapt treatment approaches.
Disclosures:
Dr Falk is Assistant Professor of Psychology in Clinical Psychiatry, and Director, Pediatric OCD, Anxiety, and Tic Disorders Program; Dr Goldman is Postdoctoral Fellow of Psychology in Psychiatry, and Dr Mohatt is Assistant Professor of Clinical Psychiatry, Vice Chair for Child and Adolescent Psychiatry, and Vice Chair, Faculty Practice, Weill Cornell Medicine, New York, NY. The authors report no conflicts of interest concerning the subject matter of this article.
References:
1. Walitza S, Melfsen S, Jans T, et al. Obsessive-compulsive disorder in children and adolescents. Deutsches Arzteblatt Int. 2011;108:173-179.
2. Bitsko R, Holbrook J, Ghandour R, et al. Epidemiology and impact of health care provider diagnosed anxiety and depression among US children. J Devel Behav Pediatr. 2018;39:395-403.
3. Bandelow B, Michaelis S. Epidemiology of anxiety disorders in the 21st century. Dial Clin Neurosci. 2015;17:327-335.
4. Goodwin GM. The overlap between anxiety, depression, and obsessive-compulsive disorder. Dial Clin Neurosci. 2015;17:249-260.
5. Rachman S. Part I: unwanted intrusive cognitions. Adv Behav Res Ther. 1981;3:89-89.
6. Walkup JT, Albano AM, Piacentini J, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. N Engl J Med. 2008;359:2753-2766
7. The Pediatric OCD Treatment Study (POTS) Team. Cognitive behavior therapy, sertraline, and their combination for children and adolescents with obsessive compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA. 2004;292):1969-1976.
8. Mohatt J, Bennett SM, Walkup JT. Treatment of separation, generalized, and social anxiety disorders in youth. Am J Psychiatry. 2014;171:741-748.
9. Strawn JR, Sakolsky DJ, Rynn MA. Psychopharmacologic treatment of children and adolescents with anxiety disorders. Child Adolesc Psychiatr Clin N Am. 2012;21:527-539.















Newsletter
Receive trusted psychiatric news, expert analysis, and clinical insights — subscribe today to support your practice and your patients.