

Publication
Article
Clozapine: Once-Daily or Divided Dosing?
Author(s):
Compared with divided dosing, patients with once-daily dosing had shorter illness duration and better clinical outcomes.


tashatuvango/AdobeStock
CASE VIGNETTE
“Jonah” is 29-year-old White male with a 4-year history of schizophrenia, with 3 psychiatric hospitalizations in the past year. He has treatment-resistant positive symptoms, including auditory and visual hallucinations, as well as persecutory delusions. Jonah has failed previous trials of oral olanzapine and risperidone as well as long-acting injectable paliperidone. He has no medical comorbidities and does not use illicit substances. His father, who is his legal guardian, is interested in a trial of clozapine. He has read that twice-a-day dosing of clozapine may reduce risk of seizure. He asks about other potential benefits of once- vs twice-daily dosing. As his outpatient psychiatrist, how would you respond?
Clozapine is the gold-standard antipsychotic for treatment-resistant schizophrenia (TRS).1 Divided daily dosing is indicated in the package insert for clozapine.2,3 This recommendation is based on elimination half-life data showing that higher nocturnal clozapine levels may increase risk of adverse effects4 and the potential for breakthrough symptoms.5 This recommendation has been challenged6 as daily bedtime dosing may reduce adverse effects such as orthostatic hypotension and daytime sedation, increase adherence, and not affect risk of seizures.7,8 However, studies comparing clozapine dose regimens and outcomes and adverse effects are limited.
The Current Study
Yang et al compared once-daily and divided clozapine dosing in terms of demographics, clinical characteristics and outcomes, and adverse effects.9 They performed a cross-sectional study in 159 patients with DSM-IV schizophrenia or schizoaffective disorder at the Institute of Mental Health in Singapore from 2016 to 2019. TRS was defined as at least 2 unsuccessful antipsychotic trials before initiation on clozapine. Exclusion criteria were current diagnosis of alcohol or non-nicotine substance dependence and history of head trauma.
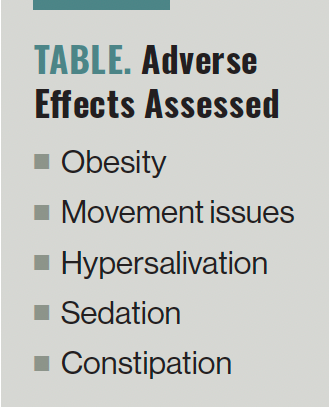
The authors collected demographic and anthropometric data. Blood clozapine and norclozapine levels were measured 12-hours post dose after an overnight fast with high-performance liquid chromatography–UV. Medical history was obtained from self-report and medical records. Psychopathology was rated by the Positive and Negative Syndrome Scale (PANSS). Functioning was assessed using the Social and Occupational Functioning Assessment Scale (SOAFAS). Neurocognition was assessed with digit sequencing and symbol coding. The adverse effects assessed can be found in the Table.


Table. Adverse Effects Assessed
Descriptive statistics were calculated based on dose regimen and compared by χ2 or Fisher exact test, Student t-test, or the Mann-Whitney U test. Multivariable regression analyses were used to assess dosing regimen and clozapine daily dose as a predictor of clinical symptoms.
Mean subject age was 40 years and 64% of the sample was male. Once-daily clozapine (at bedtime) was prescribed in 71% of participants, with a mean dose of 271 mg (range, 37.5-700 mg). Twice-daily divided clozapine was prescribed for 26% of participants, with a mean daily dose of 403 mg (range, 150-750 mg).
Participants in the once-daily dosing group were younger and had more education, shorter illness duration, fewer prior hospitalizations, and a lower daily clozapine dose. The plasma clozapine concentration corresponding to 400 mg/day was higher in the once-daily than in the divided dosing group. Patients in the once-daily dosing group were more likely to be employed and less likely to be prescribed other oral antipsychotics.
After controlling for daily clozapine dose, dosing regimen was significantly associated with PANSS total and cognitive/disorganization factor scores as well as cognitive performance scores. There was not a significant association between dosing regimen and positive or negative symptoms, SOFAS scores, or adverse effects after controlling for daily clozapine dose.
Study Conclusions
The authors concluded that most patients received clozapine once daily. Compared with divided dosing, patients with once-daily dosing had shorter illness duration and better clinical outcomes, had lower clozapine doses and corresponding plasma levels, and were more likely to be on clozapine monotherapy. There were no significant differences in clozapine-related adverse effects based on dosing regimen. Study strengths include the cumulative sample size and the broad range of demographic and clinical assessments. Study limitations include generalizability to other groups of clozapine-treated patients and absence of data on genetics, smoking, caffeine, alcohol, and inflammation. The cross-sectional nature of the study precludes evaluation of causal relationships.
The Bottom Line
Almost three-quarters of patients were prescribed clozapine as a single bedtime dose. Once-daily dosing was associated with lower daily clozapine dose, better clinical outcomes, and no significant differences in clozapine-related adverse effects. Future prospective, longitudinal studies are needed, but once-daily clozapine dosing is a viable option.
Dr Miller is a professor in the Department of Psychiatry and Health Behavior, Augusta University, Augusta, Georgia. He is on the editorial board and serves as the schizophrenia section chief for Psychiatric Times. The author reports that he receives research support from Augusta University, the National Institute of Mental Health, and the Stanley Medical Research Institute.
References
1. Buchanan RW, Kreyenbuhl J, Kelly DL, et al. The 2009 schizophrenia PORT psychopharmacological treatment recommendations and summary statements. Schizophr Bull. 2010;36(1):71-93.
2. Clozaril. Prescribing information. Novartis; 2017. Accessed January 29, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/019758s084lbl.pdf
3. Clozaril. Novartis Pharmaceuticals Canada Inc; 2011. Accessed January 29, 2024. https://www.novartis.com/ca-en/sites/novartis_ca/files/clozaril_scrip_e.pdf
4. Freudenreich O, McEvoy J. Schizophrenia in adults: guidelines for prescribing clozapine. UpToDate. 2023. Accessed January 29, 2024. https://medilib.ir/uptodate/show/14772
5. Procyshyn RM, Vila-Rodriguez F, Honer WG, Barr AM. Clozapine administered once versus twice daily: does it make a difference? Med Hypotheses. 2014;82(2):225-228.
6. Takeuchi H, Leucht S, Kane JM, et al. Antipsychotic medications: enhancing use to improve outcomes. Schizophr Bull. 2021;47(5):1201-1204.
7. Leclerc LD, Demers MF, Bardell A, et al. A chart audit study of clozapine utilization in early psychosis. J Clin Psychopharmacol. 2021;41(3):275-280.
8. Takeuchi H, Powell V, Geisler S, et al. Clozapine administration in clinical practice: once-daily versus divided dosing. Acta Psychiatr Scand. 2016;134(3):234-240.
9. Yang Z, Takeuchi H, Yee JY, et al. Once-daily versus divided dosing regimens of clozapine: a cross-sectional study in Singapore. Schizophr Res. 2023:S0920-9964(23)00354-7.
Newsletter
Receive trusted psychiatric news, expert analysis, and clinical insights — subscribe today to support your practice and your patients.
















