

News
Article
Bringing the Hospital Home: Meeting Teens in Crisis Where They Are
Learn more about a feasible, scalable, effective model of care that is a step away from the forced dichotomy of inpatient and outpatient care.


fizkes/AdobeStock

CLINICAL REFLECTIONS
Many child and adolescent psychiatrists today face 1 of 2 challenges: (1) most of your time is spent on your sickest patients in a level of care that does not offer the support you and they need, or (2) you serve patients at a level of care that is so restrictive, expensive, or removed from typical community life that one of your most therapeutic interventions is discharge. Some of this is hyperbole, but few communities have the resources to establish the robust intermediate levels of care that provide a balance between these 2 groups for both patients and their providers.
Thinking Outside of the Telehealth Box: A Model Program
Telehealth has been used for decades to enhance access to health care for rural and underserved populations. It was not until the COVID-19 pandemic that applications aimed to level other disparities. Expanded use and acceptance of telehealth has allowed for models of care that can bring far more than singular clinic visits to the home. In theory, entire departments or hospitals may operate off-site from the patient and bring their services into the home. In the same way that in-home hospice care is now universally recognized as a standard for end-of-life care—could not adolescent psychiatric hospitalization occur in the home?
This proposal has become feasible through the establishment of Bradley REACH—a fully virtual, adolescent partial hospitalization program born out of the pandemic and modeled after Emma Pendleton Bradley Hospital’s in-person programs. The first free standing psychiatric hospital for children in the US, Bradley has been a leader in intermediate levels of care with more than 7 partial programs, intensive outpatient programs (IOPs), and day treatment programs, though the care was only accessible locally in the small but urban New England town of Riverside, RI.
With individual, group, milieu, and family therapies, as well as extensive psychoeducation, medication management, and advocacy, REACH’s 3 to 5 weeklong program offers patients and families the intensity of hospitalization without the risks of inpatient admission. Small group size, low staff to patient ratio, interdisciplinary work, and a philosophy of belonging are the cornerstones of the treatment. With a clear mission to move beyond safety management typically central to intensive levels of care, the REACH program supports a more in-depth exploration of a teen’s identity, neurobiology, family system, and environment.
The REACH program, like therapeutic interventions in general, often aims to facilitate the development of a narrative for the adolescent and their family, and to share it in a way that captures belonging and the power in bearing witness to a peer’s experiences. Skilled clinicians are an invaluable part of this therapeutic exchange, and in most regions, there are not enough to meet a community’s needs.
Case Studies: Supporting Patients Where They Are
The difference between care in a community with and without intermediate levels of care is best illustrated through the teens themselves. Take “Addison,” a 16-year-old with major depressive disorder, attention-deficit/hyperactivity disorder, and 1 prior inpatient admission who now receives IOP treatment after a worsening in her anxiety in the context of a new academic year. She is prescribed fluoxetine and extended-release methylphenidate, and has had 1 prior medication trial with sertraline. Her parents work in retail. They divorced 2 years ago and shortly thereafter Addison attempted suicide. After boarding in the emergency department (ED) for several days, she was admitted to the psychiatric hospital for 2 weeks. Since that admission and step-down to partial hospitalization program (PHP) care, she has experienced resolution in suicidal thoughts. However, she continues to struggle as she navigates depression in adolescence. Her parents and outpatient providers are diligent, resourceful, and actively evaluate options and appropriate level of care with Addison. She lives in a metropolitan area in New England and has medical coverage through Medicaid.
“Kylie” is also 16, with working parents, and a history of a suicide attempt 2 years ago in the context of interpersonal loss. She has been diagnosed with disruptive mood dysregulation disorder, oppositional defiant disorder, and schizoaffective disorder. She has had multiple, 3-day involuntary inpatient psychiatric admissions, with a new medication trial each hospitalization. She is currently prescribed divalproex, quetiapine, and lurasidone and has had multiple incomplete trials of antipsychotics and mood stabilizers. Following discharge, she returns to her outpatient prescriber who is diligent and resourceful, often providing psychotherapy visits several times per month when Kylie is in crisis. Although her parents and providers work closely with one another, treatment has frequently been fragmented and interrupted by difficulty with school coordination and mandated interventions through the judicial system after being caught with a vape pen in class. Kylie lives in the suburbs in the southeast United States and has coverage through Medicaid.
Both Addison and Kylie live in moderately populous cities; have working-class, loving, conscientious parents; see dedicated, skilled providers; and are a part of the 13% of adolescent females who have attempted suicide in the past year.
Beyond Suicide Prevention
In adolescence, suicide rates continue to rise, but remain a statistically rare event. Therefore, we need to consider not just death by suicide, but the far-reaching impact of all suicidal behavior. The Centers for Disease Control and Prevention reports that for every suicide death, there were 3 hospitalizations for self-harm, 8 ED visits related to suicide, 38 self-reported suicide attempts in the past year, and 265 individuals who seriously considered suicide in the past year.1-3 Although these numbers represent adults, one could expect similar trends in adolescents.
These hospitalizations, ED visits, and incidents of self-harm give further insight into the scope of the collateral damage associated with suicidal behavior. When suicidal behavior in adolescents occurs in a vulnerable, low resource area, the impact is magnified.
Take Kylie, for example, in crisis. She has been self-harming daily but does not have a therapy visit for another 3 weeks. Her parents were unable to drive her last week, and her therapist has scheduled bimonthly because of her overextended case load. There are no intensive programs where she lives, and after her parents began to fear they were unable to keep her safe, they brought her in for an emergency evaluation. The clinician’s options were discharging home, which seemed ludicrous to all involved as that low level care was clearly not mitigating crisis, or to admit her psychiatrically. Although fraught with its own risks, and significant cost, hospitalization appeared to be the only option.
Addison, in the same situation, may have disclosed urges to self-harm at her weekly appointment. Her therapist would have the time to call parents and develop a safety plan. Later that week, if Addison activated that plan, a mobile crisis team could assist the family in de-escalation, set up an earlier follow up appointment, and navigate the intricacies of getting enrolled in an intensive program.
Addressing Disparities
The differences for Kylie and Addison intensify following placement in different levels of care. Exposure to hospitalization means higher risk of additional diagnoses and subsequent medication trials. In our experience, providers in intensive care settings, without the support or time they need, may be prone to interpret presentations as “behavioral,” “volitional,” or even antisocial. Underrepresented groups are especially prone to acquiring these labels with high-quality, outpatient, evidence-based care less commonly provided to Black and Hispanic children, leading to greater risk of developing a crisis.4 Although receiving treatment in EDs, these children experience increased utilization of pharmacologic and physical restraints relative to White children, and are more often referred for and diagnosed with agitation, aggression, and externalizing behaviors.5 These disparities and labels often come with a loss of trust in the system by patient, parent, and provider, and willingness to reveal trauma, familial stressors, and attachment difficulties may decrease.
The etiology of Addison’s intrusive fearful thoughts, irritability, and hyper-vigilance following an assault may be obvious, but even seemingly straightforward formulations can be impeded by condensed evaluation appointments and few collateral contributors. It is easy to see how Kylie reporting these same symptoms could be labeled paranoid, guarded, and preoccupied.
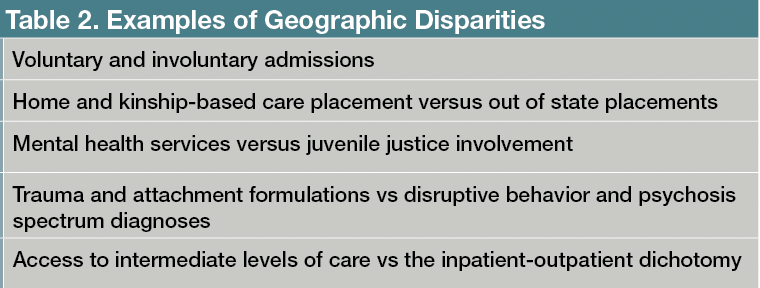
How do we explain and quantify these differences? We know that exposure to adverse childhood events, gender and sexual identity, race, ethnicity, financial stressors, and access to resources all impact the biopsychosocial presentation of an adolescent.5 Outside of the dichotomy of rural and urban, place of residence plays an indirect role. Examples of geographic disparities can be found in Table 1. This association is multifactorial but largely related to available care systems.


Table 1. Tips for Overcoming Adolescent Distrust in Telehealth
A systems of care lens illuminates the difficulties of reliance on inpatient and outpatient dichotomies. Intensive, intermediate levels of care like REACH provide an opportunity for teens and their families to connect with multiple providers in numerous treatment settings more frequently, often resulting in the formation of an intimate therapeutic alliance relatively quickly. The use of an interdisciplinary model allows for all providers on the team to focus on their clinical expertise while emphasizing the importance of building and modeling relationships. It is within the context of these relationships that treatment recommendations, understanding, validation, and education are best received.
Overcoming Obstacles and Challenges
While the benefits of virtual care greatly outweigh the cons, new challenges present themselves when expanding to diverse communities. Expansion into Florida, for example, has presented both predictable and unforeseen hurdles that both caregivers and clinicians have had to adapt to.
Virtual care means access to stable internet is not only imperative, but necessary. This has been one of the largest areas of need not only because of untenable cost for many of these families, but also because REACH serves families in areas so remote and underdeveloped, internet access is often not available or sustainable. Clinicians have had to actively problem solve, work with schools and area providers, and utilize community resources to assist with payment of internet for the duration of treatment, on top of finding a private space for teens to join programs that may not be within their home. After working with several of these families, clinicians and team members are proactively involved in grant applications and alternative funding sources to purchase tablets that can be distributed to teens and families that may not be able to purchase one themselves.
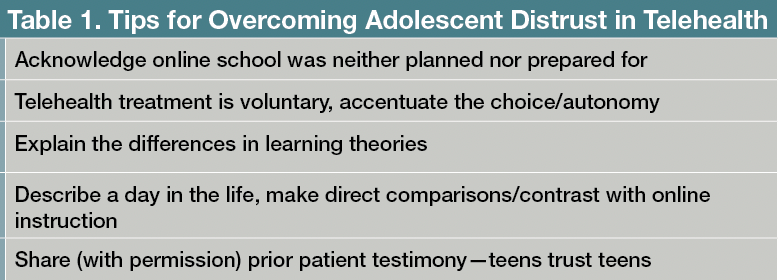
Moving into new communities also means adapting to regional norms and expectations surrounding the treatment of psychiatric illness. In Florida, for example, psychiatric admission of minors is pursued involuntarily as the rule rather than the exception. Although this approach is largely related to interpretations of age of consent, the involuntary nature of first exposure to treatment further highlights the trauma and stigma associated with treatment of serious mental health conditions in children. Often coupled with a lack of community support and resources, our teams are challenged with treatment starting at a very different point. Clinically, we must begin with a greater emphasis on rapport building; providing ongoing psychoeducation on mental health in teens; and disbarring assumptions about teen mental health, therapy, and medications, all while gaining and building trust through a screen. Tips for overcoming patient distrust of telehealth can be found in Table 2.


Table 2. Examples of Geographic Disparities
Common questions surrounding the nature of a virtual relationship typically arise in 3 categories: engagement, effectiveness, and safety. Virtual schooling brought near universal exposure to spending time on screen; however, this experience has frequently deterred families from virtual care more than supported it. Prior to admission, an intake assessment and introduction to the program serve as the starting point to identifying barriers. Outside of the logistics, anxiety, inattention, and boredom tend to top the list of challenges to engagement. Skilled direct care staff serve as our primary intervention and spend the entirety of the program day with patients to develop meaningful, individual relationships that can then appeal to teen’s interests. Direct care staff are approachable, foster a primary treatment component of connectedness, and importantly, are always included in the daily treatment team meeting. Supporting direct care staff and creating a team that makes space for a nonhierarchical approach to care allows the PHP team to function interdependently, effectively, and with a sense of joint purpose. In addition, as relationships form amongst the teens and staff, attention is paid to group needs, common threads of interest and other opportunities for developing a sense of belonging. Finally, treatment of attention and disruptive behavior disorders is often prioritized to facilitate the teen’s ability to participate.
Assessing Efficacy and Success
Defining effectiveness has looked different in each region, which is a function of both the resources available and operation of the system. We have found a focus on patient and parent-centered outcomes that address quality of life and functional status to improve from admission to discharge. Further work must be done in partnership with payors and systems to establish PHP cost-savings and impact on stakeholder’s including child and family services, schools, and juvenile justice.
Given that most of our PHP patients are at relatively high risk for self-harm, readmission, and suicide, safety is of utmost importance. Again, a team centered approach is imperative, with multiple opportunities for group and individual assessments by multiple providers each day. In the rare case where safety is of imminent concern, the virtual platform is used to create a separate “break out room” for additional support, team planning and de-escalation. Caregivers, individual therapists, and others can be seamlessly brought together with the patient within minutes for processing, behavioral chain analyses, supported coping strategies, and safety planning.
In addition to decreasing need for extended inpatient admissions, REACH works to maintain the safety of a teen in the least restrictive setting possible to facilitate successful reentry into the community. School systems play an integral role in this transition, and understanding the differences across states and regions has been imperative to effectively partnering with schools. An individual school’s policies may vary greatly in terms of approach to medical absences, for example, and most often our clinicians find that detailing how PHP can address some of the prior issues at school before the student’s return is the key to an impactful partnership. Additionally, our lead clinicians allot defined times to connect with schools to provide education on mental health and its impact on a teen’s day to day. Modeling advocacy for caregivers and teens and demonstrating the power of collaboration serves not only to build trust, but to strengthen supports in the teen’s life following discharge.
There Is Hope
Serendipitously, a PHP opened in Kylie’s state, with a fully virtual program so her parents would not have to worry about daily transportation. At first, she thought it would not be a good fit for her. She had hated virtual school during the pandemic and her parents noted her mood was even worse at this time, not to mention her grades. But after her third hospitalization and sixth medication trial, she and her family were willing to try anything. The first few days were tough. Several hours of interviews, information gathering, and introductions made up more time spent on mental health treatment in 1 week than in the prior year. Groups were awkward at first. Kylie wondered when she should unmute to share, what her peers would think of her and how she could sustain her attention on a computer all day.
She quickly realized most of the group felt the same way. There was time to bond. She shared a lot of interests with her peers in group and noticed how many of their issues at home and school aligned. She gained confidence sharing and began to feel close with her treatment group. Kylie shared her concerns for her upcoming family sessions with her peers and they provided encouragement and reflected on ways they handled similar situations. She prepared for school meetings with her individual therapist and detailed her school avoidance and her parents’ frustration with her in process group.
Upon discharge, Kylie’s PHP providers were able to coordinate care with her outpatient providers, pediatricians, and school system to ensure a smooth transition back into daily life. They helped with diagnostic clarification and used this to support her detailed history of ongoing struggles within school. Her providers, teachers, and family were better able to understand her mental health struggles and were educated to understand interventions that worked for Kylie and those that did not. Within 4 weeks, Kylie received more than double the hours of treatment she would have otherwise received in a year of outpatient care.
A single Bradley REACH PHP treatment team can treat up to 156 teens per year. It would take more than 5 new therapists hired to each city to see the same number of patients in a much less intensive level of care.
PHPs aim to be a catalyst for change in struggling communities. While most intermediate levels of care are necessary in a robust behavioral healthcare system, a virtual PHP is uniquely situated as a quickly scalable option. IOPs, which typically lack prescribers, intensive family work, and a cohesive teen group have the opportunity for similar scaling, but lack the intensity necessary for intensive medication management and development of the therapeutic milieu.
Dozens of otherwise modern cities have no intermediate levels of psychiatric care for adolescents. In an ideal world, every city would have the leaders, capacity, funds, and support to develop a system of care that includes school-based services, wrap-around care, IOPs, day treatment models, mobile crisis services, and PHPs. That ideal is unlikely to come to fruition in many regions for a variety of reasons that may prove too difficult for health care providers and administrators to tackle. However, the Bradley REACH virtual PHP has demonstrated a feasible, scalable, effective model of care that is a step away from the forced dichotomy of inpatient and outpatient care.
Dr Gibson is a psychiatrist with Bradley REACH, clinical instructor in the Department of Psychiatry and Human Behavior at the Warren Alpert Medical School of Brown University,and serves as regional president for the Pittsburgh chapter of the American Academy of Child & Adolescent Psychiatry. Ms Chaudhrey is a clinical social worker and team lead with the REACH all-virtual adolescent partial program at Bradley Hospital.
References
1. Introduction to the HCUP National Impatient Sample (NIS). Healthcare Cost and Utilization Project; Agency for Healthcare Research and Quality. 2020. Accessed April 16, 2024.www.hcup-us.ahrq.gov/db/nation/nis/NIS_Introduction_2020.jsp
2. Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS). Updated November 8, 2023. Accessed April 16, 2024. www.cdc.gov/injury/wisqars
3. 2021 NSDUH Annual National Report. Substance Abuse and Mental Health Services Administration. January 4, 2023. Accessed April 16, 2024. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report
4. Abrams AH, Badolato GM, Boyle MD, et al. Racial and ethnic disparities in pediatric mental health-related emergency department visits. Pediatr Emerg Care. 2022;38(1):e214-e218.
5. Hoffmann JA, Alegría M, Alvarez K, et al. Disparities in pediatric mental and behavioral health conditions. Pediatrics. 2022;150(4):e2022058227.
Newsletter
Receive trusted psychiatric news, expert analysis, and clinical insights — subscribe today to support your practice and your patients.
















